Can a Baby With Hydrocephalus Lead a Normal Life?
Contents
- What is hydrocephalus
-
- Ventricles and Cerebrospinal Fluid
- Hydrocephalus types and classification
- Hydrocephalus in adults
- Hydrocephalus causes
- Common causes of Congenital Hydrocephalus
- Mutual causes of Acquired Hydrocephalus
- Adventure factors for hydrocephalus
- Newborns
- Other contributing factors
- Hydrocephalus prevention
- Hydrocephalus life expectancy
- Hydrocephalus prognosis
- Hydrocephalus complications
- Hydrocephalus symptoms
-
- Infants
- Toddlers and older children
- Young and Center Aged Adults
- Older Adults (normal pressure level hydrocephalus)
-
- Hydrocephalus diagnosis
- Normal force per unit area hydrocephalus
- Hydrocephalus handling
- Hydrocephalus shunt
- What problems can occur with hydrocephalus shunts?
- Shunt infection
- Shunt alert cards
- Additional treatments
- Endoscopic Third Ventriculostomy
- Complications of endoscopic 3rd ventriculostomy
- Hydrocephalus Shunt and Endoscopic Third Ventriculostomy Complications
- Normal pressure hydrocephalus
- Coping and back up
- Hydrocephalus shunt
-
What is hydrocephalus
Hydrocephalus is a serious condition characterized by excessive accumulation of cerebrospinal fluid (CSF) in the brain. In babies, hydrocephalus (fluid accumulation in the brain) tin can cause the babies' head to abound unusually quickly. Hydrocephalus may also result in jutting fontanelles, or a bulging area at the soft spot at the top of the infant's head. In adults, hydrocephalus causes neurological problems such every bit drowsiness, seizures, unstable balance, poor coordination, difficulty walking, gait disturbances, impaired vision, memory loss and urinary urgency or incontinence.
Hydrocephalus is a condition, not a disease. Information technology can develop for a variety of reasons, sometimes as office of another status.
- The incidence of built (nowadays at birth) hydrocephalus is approximately three for every 1000 live births.
- The incidence of developed hydrocephalus depends on the frequency of precipitating causes, such every bit brain infections and and then forth. Hydrocephalus is estimated to affect 1 in every 10,000 people at some indicate in their lifetime.
- The incidence of hydrocephalus in males and females is roughly equal. Peak incidence occurs in infancy and machismo.
The excessive accumulation of cerebrospinal fluid (CSF) results in an abnormal widening of spaces in the encephalon called ventricles (run into Figures 1 – 3). This widening creates potentially harmful force per unit area on the tissues of the brain.
The ventricular system is fabricated upwards of four ventricles connected past narrow passages (see Effigy 1). Commonly, cerebrospinal fluid (CSF) flows through the ventricles, exits into cisterns (airtight spaces that serve equally reservoirs) at the base of the brain, bathes the surfaces of the brain and spinal cord, and and then reabsorbs into the bloodstream.
Cerebrospinal fluid (CSF) has 3 of import life-sustaining functions:
- To keep the brain tissue buoyant, acting as a cushion or "shock absorber";
- To act as the vehicle for delivering nutrients to the encephalon and removing waste matter; and
- To flow betwixt the attic and spine and compensate for changes in intracranial blood volume (the amount of blood within the brain).
The balance betwixt product and absorption of CSF is critically important. Considering CSF is fabricated continuously, medical weather that block its normal flow or absorption will result in an over-accumulation of CSF. The resulting pressure of the fluid confronting brain tissue is what causes hydrocephalus.
The number of people who develop hydrocephalus or who are currently living with it is difficult to plant since the condition occurs in children and adults, and can develop later in life. A 2008 data review by the University of Utah plant that, in 2003, hydrocephalus accounted for 0.6 percent of all pediatric infirmary admissions in the The states. Some estimates written report 1 to two of every one,000 babies are built-in with hydrocephalus. Over 1,000,000 people in the United States currently alive with hydrocephalus.
If hydrocephalus remains untreated the intracranial pressure will rise eventually resulting in compression of the brain stem and subsequently expiry from respiratory causes.
Hydrocephalus is the well-nigh common reason for brain surgery in children.
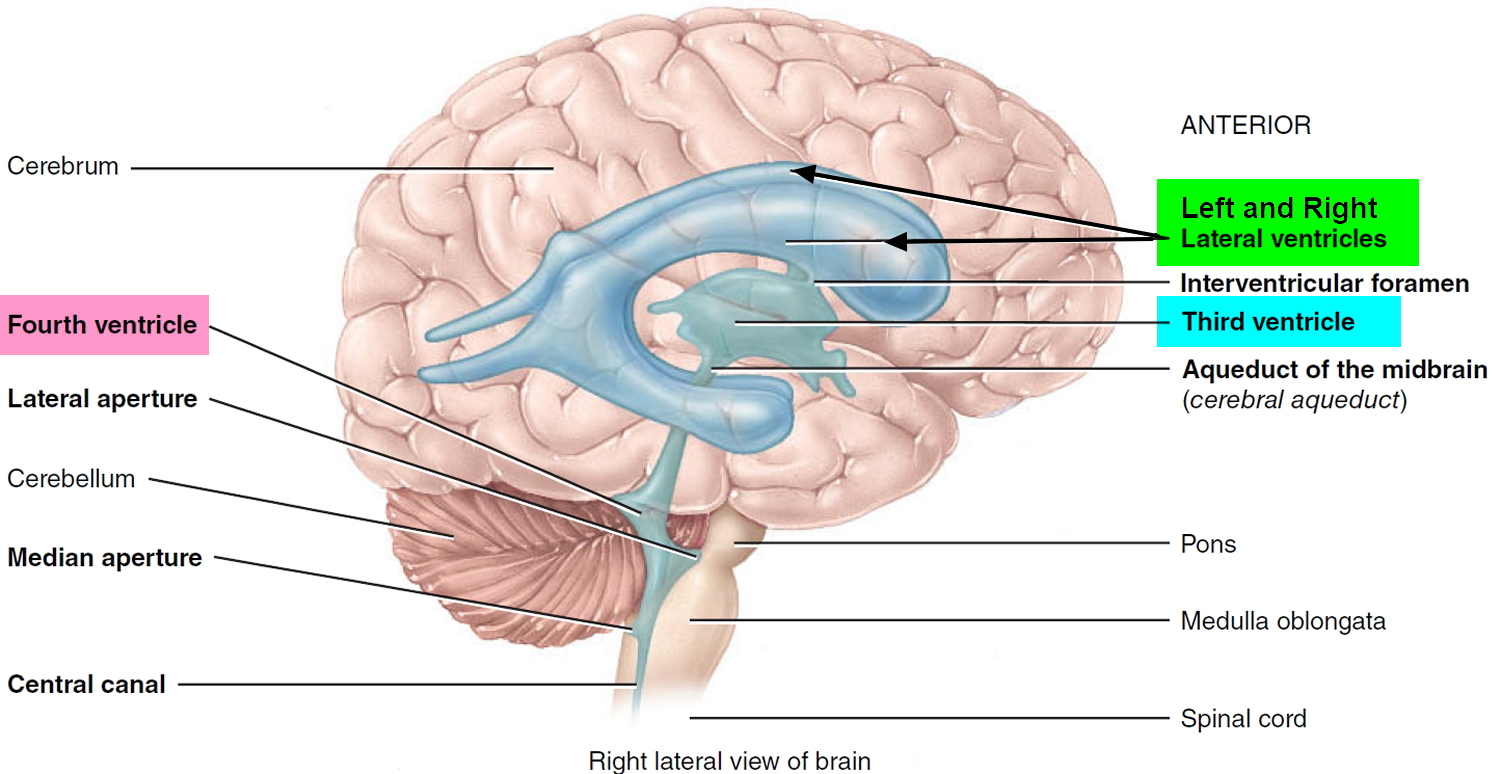
Ventricles and Cerebrospinal Fluid
The brain has four internal chambers called ventricles. The largest and nearly frontal ones are the ii lateral ventricles, which course an arc in each cerebral hemisphere. Through a tiny pore chosen the interventricular foramen, each lateral ventricle is continued to the third ventricle, a narrow median space inferior to the corpus callosum. From here, a culvert called the cerebral aqueduct passes downwards the core of the midbrain and leads to the fourth ventricle, a modest triangular chamber between the pons and cerebellum. Caudally, this infinite narrows and forms a central canal that extends through the medulla oblongata into the spinal cord.
Effigy ane. Ventricles of the brain
On the floor or wall of each ventricle is a spongy mass of blood capillaries called a choroid plexus, named for its histological resemblance to a fetal membrane called the chorion. Ependyma, a type of neuroglia that resembles a cuboidal epithelium, lines the ventricles and canals and covers the choroid plexuses. It produces cerebrospinal fluid (CSF).
Cerebrospinal fluid is a clear, colorless liquid that fills the ventricles and canals of the CNS and bathes its external surface. The brain produces near 500 mL of cerebrospinal fluid per day, but the fluid is constantly reabsorbed at the same rate and only 100 to 160 mL is usually present at one fourth dimension. Almost forty% of it is formed in the subarachnoid space external to the encephalon, 30% by the general ependymal lining of the brain ventricles, and thirty% by the choroid plexuses. Cerebrospinal fluid production begins with the filtration of blood plasma through the capillaries of the brain. Ependymal cells modify the filtrate as it passes through them, so the cerebrospinal fluid has more sodium chloride than claret plasma, but less potassium, calcium, and glucose and very fiddling protein.
Cerebrospinal fluid serves three functions for the brain:
- Buoyancy. Because the brain and cerebrospinal fluid are similar in density, the brain neither sinks nor floats in the cerebrospinal fluid. Information technology hangs from delicate specialized fibroblasts of the arachnoid meninx. A human brain removed from the body weighs most one.5 kg, but when suspended in cerebrospinal fluid its effective weight is simply about fifty thousand. This buoyancy allows the encephalon to attain considerable size without existence impaired past its own weight. If the brain rested heavily on the floor of the cranium, the pressure level would kill the nervous tissue.
- Protection. Cerebrospinal fluid also protects the brain from hit the cranium when the head is jolted. If the jolt is severe, however, the brain however may strike the inside of the cranium or suffer shearing injury from contact with the athwart surfaces of the cranial flooring. This is ane of the common findings in caput injuries (concussions) from contact sports like NFL, rugby and boxing.
- Chemic stability. Cerebrospinal fluid rinses metabolic wastes from the nervous tissue and regulates its chemic environment. Slight changes in cerebrospinal fluid composition tin can cause malfunctions of the nervous system. For example, a loftier glycine concentration disrupts the control of body temperature and claret force per unit area, and a high pH causes dizziness and fainting.
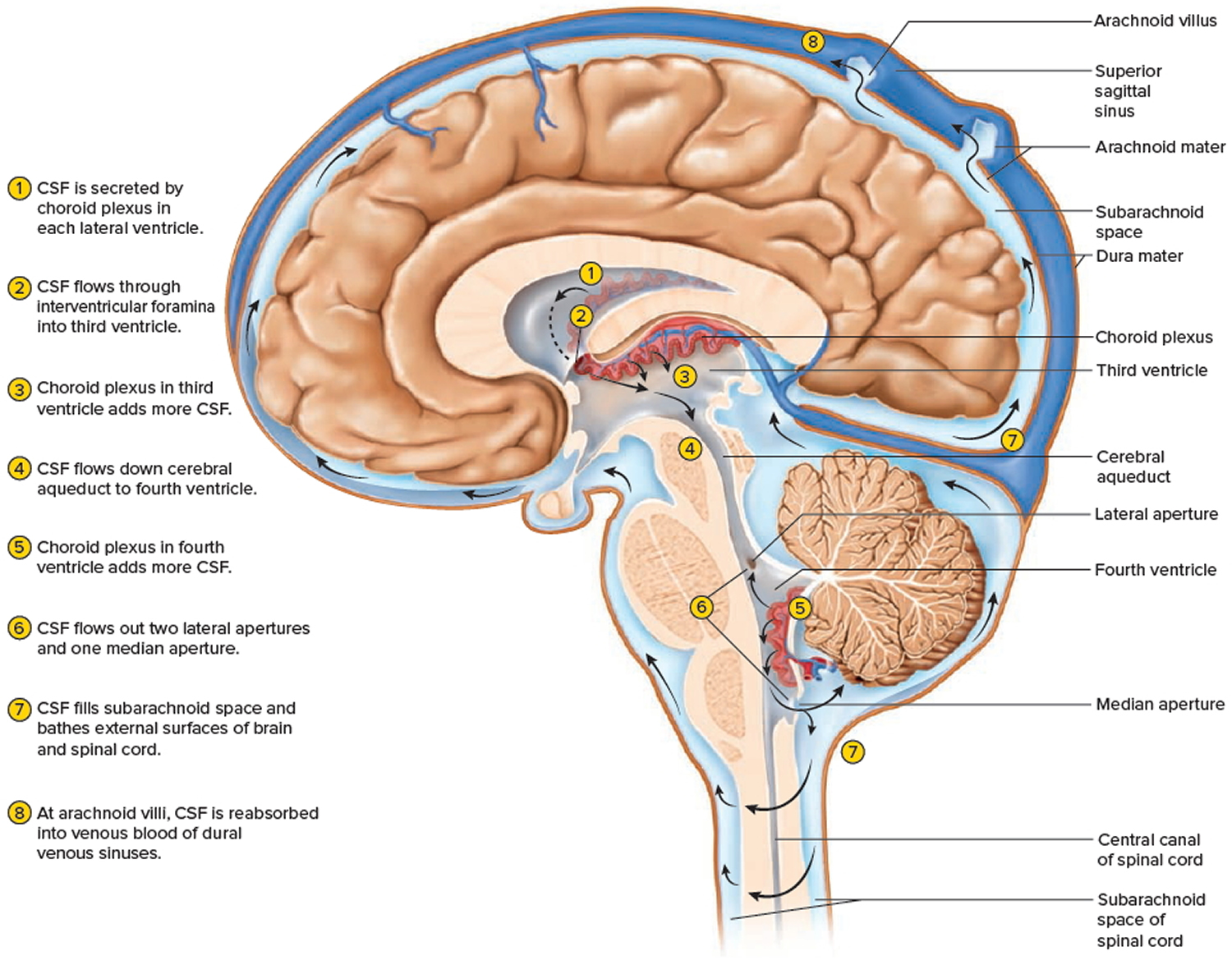
Cerebrospinal fluid continually flows through and around the encephalon and spinal cord, driven partly past its own pressure, partly by the beating of ependymal cilia, and partly by rhythmic pulsations of the brain produced past each heartbeat. The cerebrospinal fluid of the lateral ventricles flows through the interventricular foramina into the tertiary ventricle, then down the cerebral aqueduct to the fourth ventricle. The third and 4th ventricles and their choroid plexuses add more than cerebrospinal fluid along the way. A small amount of cerebrospinal fluid fills the central canal of the spinal cord, simply ultimately, all of information technology escapes through three pores in the fourth ventricle—a median aperture and two lateral apertures. These pb into the subarachnoid infinite on the encephalon and spinal cord surface. From here, cerebrospinal fluid is reabsorbed past arachnoid granulations, extensions of the arachnoid meninx shaped similar niggling sprigs of cauliflower, protruding through the dura mater into the superior sagittal sinus. Cerebrospinal fluid penetrates the walls of the granulations and mixes with claret in the sinus.
Figure 2. Cerebrospinal fluid formation, absorption and circulation around and within the brain
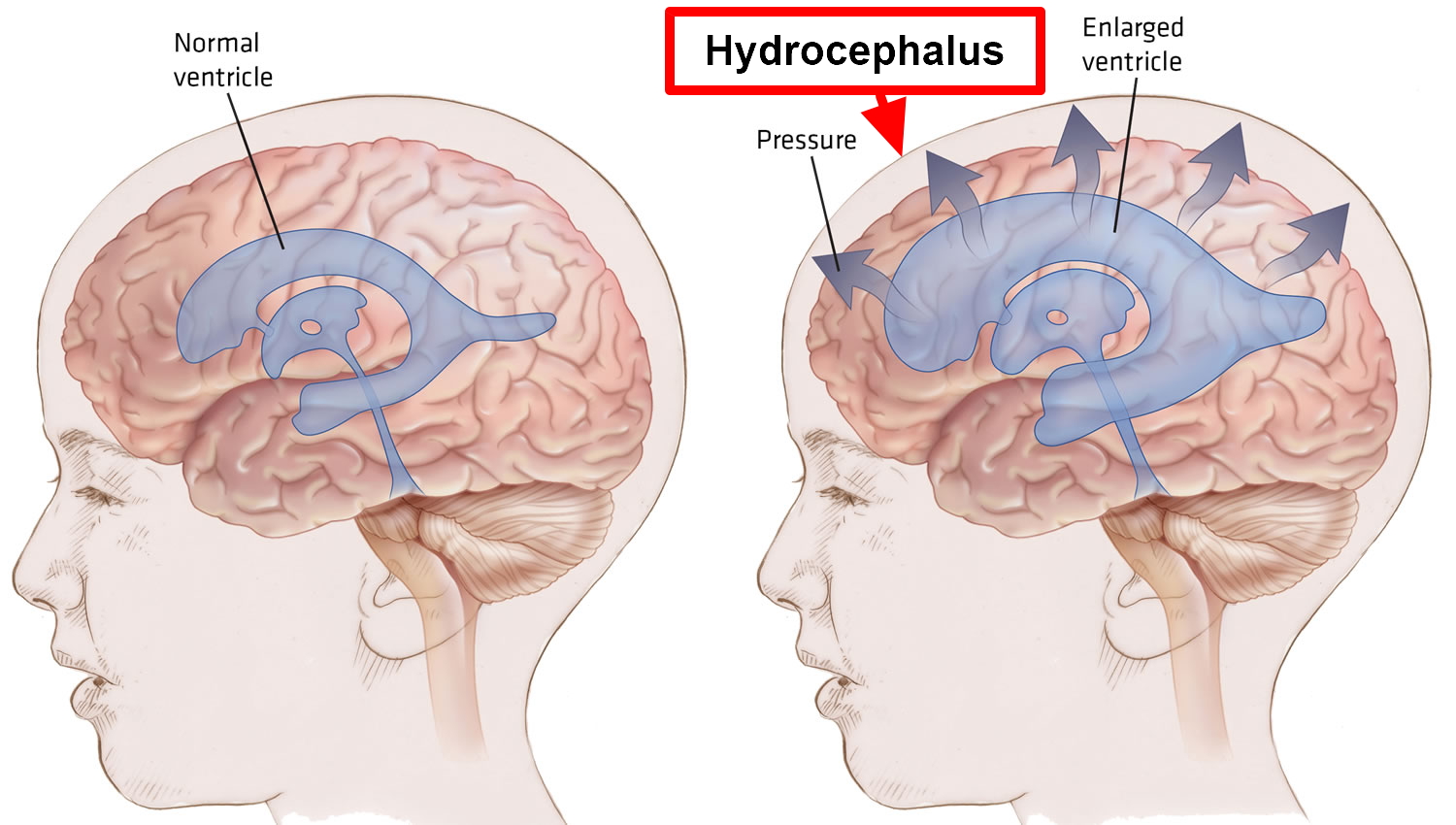
 Effigy 3. Hydrocephalus
Effigy 3. Hydrocephalus
Hydrocephalus types and classification
Hydrocephalus may exist built or acquired.
- Congenital hydrocephalus is present at birth and may exist caused by either events or influences that occur during fetal development, or genetic abnormalities. Congenital hydrocephalus is now often diagnosed before birth through routine ultrasound. The incidence of built hydrocephalus is approximately iii for every one thousand live births.
- Acquired hydrocephalus develops at the fourth dimension of birth or at some point subsequently. This type of hydrocephalus can affect individuals of all ages and may exist caused by head trauma, brain tumor, cyst, intraventricular hemorrhage or infection of the central nervous system.
Hydrocephalus may also exist communicating or non-communicating.
- Communicating hydrocephalus. If the cerebrospinal fluid (CSF) flows freely throughout the encephalon's ventricular system and the subarachnoid infinite, information technology is referred to every bit communicating hydrocephalus. Communicating hydrocephalus is the result of defective absoprtion of cerebrospinal fluid (CSF) and/or increased product (rare).
- Non-communicating hydrocephalus — besides chosen "obstructive" hydrocephalus — occurs when the flow of CSF is blocked forth i or more of the narrow passages connecting the ventricles. One of the most mutual causes of hydrocephalus is "aqueductal stenosis." In this case, hydrocephalus results from a narrowing of the aqueduct of Sylvius (cerebral channel), a modest passage betwixt the 3rd and 4th ventricles in the middle of the brain. Obstruction may be caused by a diversity of things including mass lesions such as brain tumors or cysts.
Hydrocephalus in adults
There are two other forms of hydrocephalus which do not fit exactly into the categories mentioned to a higher place and primarily impact adults: hydrocephalus ex-vacuo and normal pressure level hydrocephalus.
- Hydrocephalus ex-vacuo occurs when stroke or traumatic injury cause harm to the brain. In these cases, brain tissue may actually compress.
- Normal pressure hydrocephalus occurs in older adults (most often affects people over the age of sixty) when the ventricles of the brain are enlarged, but at that place is footling or no increase in the pressure within the ventricles. Sometimes the cause of normal pressure hydrocephalus is known – that may result from a subarachnoid hemorrhage, head trauma, infection, tumor, or complications of surgery. Only most often normal force per unit area hydrocephalus is idiopathic, which means the crusade is not known. It is estimated that more than 700,000 Americans have normal force per unit area hydrocephalus, but less than xx% receive an advisable diagnosis. Normal pressure hydrocephalus occurs due to reduced absorption of the CSF. However, the exact machinery of normal pressure hydrocephalus is unknown. Normal pressure hydrocephalus develops insidiously. In fact, over the time the lateral ventricles (CSF filled cavity in the middle of the brain) in the brain gradually enlarge just with little increase in CSF pressure level. Because of this, at that place is stretching and distortion of the brain tissue. Specifically, the office of the brain that is distorted contains nerve fibers that innervate the legs and bladder, hence explaining the gait and bladder problems in normal pressure hydrocephalus. Dementia occurs due to distortion of the brain tissue surrounding the ventricles.Mobility issues, dementia and urinary incontinence are the main symptoms of normal pressure hydrocephalus, but because they come on gradually and are similar to the symptoms of other, more mutual conditions, such as Alzheimer's illness, it can exist hard to diagnose. It's important to diagnose normal force per unit area hydrocephalus correctly because, unlike Alzheimer's illness, the symptoms can exist relieved with treatment.
- Prognosis of Normal pressure hydrocephalusThe major inability acquired past normal pressure hydrocephalus is progressive dementia, and information technology is of import to recognize normal pressure level hydrocephalus every bit a cause of dementia because it is potentially treatable. While dementia caused by other diseases (such as Alzheimer's disease and Parkinson's disease) volition take on a slowly progressive class, with treatment of normal pressure hydrocephalus the dementia can be improved or even reversed. Considering that, the prognosis of normal pressure hydrocephalus is better than other causes of dementia.
Hydrocephalus causes
Hydrocephalus is caused by an imbalance between how much cerebrospinal fluid is produced and how much is absorbed into the bloodstream.
The causes of hydrocephalus are withal non well understood. Hydrocephalus may result from inherited genetic abnormalities (such as the genetic defect that causes aqueductal stenosis) or developmental disorders (such as those associated with neural tube defects including spina bifida and encephalocele). Other possible causes include complications of premature birth such as intraventricular hemorrhage, diseases such as meningitis, tumors, traumatic caput injury, or subarachnoid hemorrhage, which block the get out of CSF from the ventricles to the cisterns or eliminate the passageway for CSF within the cisterns.
Excess cerebrospinal fluid in the ventricles occurs for one of the following reasons:
- Obstruction. The most common trouble is a fractional obstacle of the normal flow of cerebrospinal fluid, either from one ventricle to another or from the ventricles to other spaces around the brain.
- Poor absorption. Less mutual is a problem with the mechanisms that enable the claret vessels to blot cerebrospinal fluid. This is oft related to inflammation of brain tissues from affliction or injury.
- Overproduction. Rarely, cerebrospinal fluid is created more speedily than it tin exist absorbed.
Common causes of Congenital Hydrocephalus
- Aqueductal stenosis – The virtually common cause of congenital hydrocephalus is an obstruction called aqueductal stenosis. This occurs when the long, narrow passageway between the tertiary and 4th ventricles (the aqueduct of Sylvius = cerebral aqueduct) is narrowed or blocked, perhaps considering of infection, hemorrhage, or a tumor. Fluid accumulates "upstream" from the obstruction, producing hydrocephalus.
- Neural tube defect – Some other common cause of hydrocephalus is a neural tube defect. An open up neural tube defect, where the spinal string is exposed at nativity and is often leaking CSF, is called a myelomeningocele, and is often referred to as spina bifida. This kind of neural tube defect ordinarily leads to the Chiari Two malformation, which causes part of the cerebellum and the 4th ventricle to push downwardly through the opening at the base of the skull into the spinal cord surface area, blocking CSF flow out of the fourth ventricle and causing hydrocephalus.
- Arachnoid cysts – Congenital hydrocephalus can also exist caused past arachnoid cysts, which may occur anywhere in the brain. In children, they're frequently located at the back of the brain (posterior fossa) and in the area of the third ventricle. These cysts are filled with CSF and lined with the arachnoid membrane, ane of the iii meningeal coverings. Some arachnoid cysts are self-independent, while others are connected with the ventricles or the subarachnoid space. The fluid trapped past the cysts may block the CSF pathways, causing hydrocephalus.
- Keen-Walker syndrome – In Nifty-Walker syndrome, some other cause of congenital hydrocephalus, the fourth ventricle becomes enlarged because its outlets are partly or completely closed and part of the cerebellum fails to develop. Smashing-Walker syndrome may also exist associated with abnormal development in other parts of the encephalon and sometimes leads to aqueductal stenosis. In some instances, 2 shunts are placed in the child'south ventricles — one in the lateral ventricle and another in the 4th ventricle to manage the hydrocephalus.
- Chiari malformation – There are ii types of Chiari malformation. Both types occur in the bottom of the brain stem where the brain and spinal cord join. The lowest portion of the brain is displaced and is lower than normal pushing downwardly into the spinal column.
Congenital hydrocephalus can be caused past a condition such as spina bifida, or an infection the mother develops during pregnancy, such as mumps or rubella (German measles).
Information technology'due south estimated spina bifida affects one infant in every 700 born in United States. Most of them will have hydrocephalus.
Many babies born with hydrocephalus (built hydrocephalus) take permanent brain damage.
This can cause a number of long-term complications, such as:
- learning disabilities
- impaired speech
- memory problems
- short attention bridge
- problems with organizational skills
- vision problems, such as a squint and visual harm
- problems with physical co-ordination
- epilepsy
If your kid has learning disabilities, they'll need extra back up from their nursery or school to ensure their needs are being met.
Common causes of Acquired Hydrocephalus
- Intraventricular hemorrhage – An intraventricular hemorrhage, which most frequently affects premature newborns, may crusade an caused class of hydrocephalus. When small claret vessels alongside the ventricular lining rupture, claret may block or scar the ventricles or plug the arachnoid villi, which permit CSF to be absorbed. When the CSF can't exist absorbed, hydrocephalus results.
- Meningitis – Meningitis is an inflammation of the membranes of the encephalon and spinal cord. Acquired past a bacterial or (less frequently) viral infection, meningitis can scar the fragile membranes called meninges that line the CSF pathway. An acquired form of hydrocephalus may develop if this scarring obstructs the flow of CSF as it passes through the narrow ventricles or over the surfaces of the brain in the subarachnoid space.
- Head injury – A head injury tin damage the encephalon'south tissues, nerves, or blood vessels. Claret from ruptured vessels may enter the CSF pathway, causing inflammation. Sites of CSF absorption might then be blocked by scarred membranes – meninges – or past blood cells. The CSF flow is restricted, and hydrocephalus develops.
- Brain tumors – In children, encephalon tumors almost commonly occur in the back of the brain which is referred to equally the posterior fossa. Every bit a tumor grows, it may fill up or compress the fourth ventricle, blocking the flow of CSF and causing hydrocephalus. A tumor somewhere else in the brain might likewise cake or shrink the ventricular organisation.
Risk factors for hydrocephalus
In many cases, the exact event leading to hydrocephalus is unknown. However, a number of developmental or medical problems can contribute to or trigger hydrocephalus.
Newborns
Hydrocephalus nowadays at nativity (congenital) or shortly after birth may occur considering of any of the following:
- Abnormal evolution of the cardinal nervous system that can obstruct the menstruation of cerebrospinal fluid
- Bleeding within the ventricles, a possible complication of premature birth
- Infection in the uterus during a pregnancy, such as rubella or syphilis, that can cause inflammation in fetal brain tissues
Other contributing factors
Other factors that tin contribute to hydrocephalus amid any age group include:
- Lesions or tumors of the brain or spinal cord
- Primal nervous system infections, such as bacterial meningitis or mumps
- Bleeding in the brain from a stroke or caput injury
- Other traumatic injury to the brain.
Hydrocephalus prevention
Hydrocephalus isn't a preventable condition. However, there are ways to potentially reduce the risk of hydrocephalus:
- If yous're pregnant, get regular prenatal intendance. Following your doctor's recommended schedule for checkups during pregnancy can reduce your adventure of premature labor, which places your baby at risk of hydrocephalus and other complications.
- Protect against infectious illness. Follow the recommended vaccination and screening schedules for your age and sex. Preventing and promptly treating the infections and other illnesses associated with hydrocephalus may reduce your take chances.
To foreclose head injury:
- Utilise appropriate condom equipment. For babies and children, use a properly installed, age- and size-appropriate child safety seat on all automobile trips. Brand sure all your baby equipment — crib, stroller, swing, highchair — meets all rubber standards and is properly adapted for your baby's size and development. Children and adults should wear helmets while riding bicycles, skateboards, motorcycles, snowmobiles or all-terrain vehicles.
- Ever wear a seat belt in a motor vehicle. Small children should be secured in child prophylactic seats or booster seats. Depending on their size, older children may exist adequately restrained with seat belts.
Should you be vaccinated against meningitis?
Inquire your doctor if yous or your child should receive a vaccine against meningitis, once a common cause of hydrocephalus. The Centers for Disease Command and Prevention recommends meningitis vaccination for preteen children and boosters for teenagers. It'due south likewise recommended for younger children and adults who may be at increased risk of meningitis for whatever of the following reasons:
- Traveling to countries where meningitis is common
- Having an immune system disorder called terminal complement deficiency
- Having a damaged spleen or having had the spleen removed
- Living in a college dormitory
- Joining the armed services
Hydrocephalus life expectancy
The life expectancy for individuals diagnosed with hydrocephalus is difficult to predict, although in that location is some correlation between the specific cause of the hydrocephalus and the outcome. Prognosis is further clouded by the presence of associated disorders, the timeliness of diagnosis, and the success of treatment. The degree to which relief of CSF pressure level following shunt surgery tin can minimize or reverse damage to the brain is not well understood.
Affected individuals and their families should be aware that hydrocephalus poses risks to both cognitive and physical evolution. However, many children diagnosed with the disorder do good from rehabilitation therapies and educational interventions and keep to lead normal lives with few limitations. Handling by an interdisciplinary squad of medical professionals, rehabilitation specialists, and educational experts is critical to a positive outcome. Left untreated, progressive hydrocephalus may be fatal.
The symptoms of normal pressure hydrocephalus unremarkably go worse over fourth dimension if the condition is not treated, although some people may experience temporary improvements. While the success of treatment with shunts varies from person to person, some people recover virtually completely after treatment and have a good quality of life. Early diagnosis and treatment improves the risk of a expert recovery.
Hydrocephalus prognosis
The prognosis is dependent on the underlying cause. The outlook is particularly poor for untreated hydrocephalus in infants; these often outcome in infection and death.
A pocket-sized number will survive to childhood, but take some caste of intellectual handicap and developmental bug. The outlook is good for infants with treated not-tumor related hydrocephalus – 70% will maintain a normal IQ and attend normal school.
Damage already sustained tends to be permanent – loss of cerebral office may pesist even after treatment as may visual loss.
Hydrocephalus complications
Long-term complications of hydrocephalus can vary widely and are often hard to predict.
If hydrocephalus has progressed past the time of nativity, it may result in significant intellectual, developmental and physical disabilities. Less severe cases, when treated appropriately, may take few, if any, serious complications.
Adults who have experienced a significant reject in memory or other thinking skills by and large have poorer recoveries and persistent symptoms later treatment of hydrocephalus.
The severity of complications depends on:
- Underlying medical or developmental bug
- Severity of initial symptoms
- Timeliness of diagnosis and treatment
Hydrocephalus symptoms
Symptoms of hydrocephalus vary with age, disease progression, and individual differences in tolerance to the condition. For example, an infant'southward ability to compensate for increased CSF pressure and enlargement of the ventricles differs from an developed'south. The infant skull can expand to accommodate the buildup of CSF because the sutures (the fibrous joints that connect the bones of the skull) have not yet closed.
In infancy, the most obvious indication of hydrocephalus is often a rapid increment in caput circumference or an unusually large head size. Other symptoms may include vomiting, sleepiness, irritability, downward difference of the eyes (also called "sun setting"), and seizures.
Older children and adults may feel different symptoms considering their skulls cannot expand to adapt the buildup of CSF. Symptoms may include headache followed by airsickness, nausea, blurred or double vision, sunday setting of the optics, issues with residuum, poor coordination, gait disturbance, urinary incontinence, slowing or loss of developmental progress, lethargy, drowsiness, irritability, or other changes in personality or noesis including retention loss.
Symptoms of normal pressure hydrocephalus include problems with walking, impaired float control leading to urinary frequency and/or incontinence, and progressive mental impairment and dementia. An individual with this blazon of hydrocephalus may have a general slowing of movements or may complain that his or her anxiety feel "stuck." Because some of these symptoms may besides exist experienced in other disorders such equally Alzheimer's disease, Parkinson'due south disease, and Creutzfeldt-Jakob disease, normal pressure hydrocephalus is ofttimes incorrectly diagnosed and never properly treated. Doctors may use a diversity of tests, including brain scans such as computed tomography (CT) and magnetic resonance imaging (MRI), a spinal tap or lumbar catheter, intracranial pressure level monitoring, and neuropsychological tests, to assistance them accurately diagnose normal pressure hydrocephalus and rule out any other conditions.
The symptoms described in this section account for the most typical means in which progressive hydrocephalus is noticeable, but it is important to call up that symptoms vary significantly from person to person.
The symptoms of untreated hydrocephalus vary. During pregnancy, routine ultrasound can detect enlarged ventricles or spaces within a babe's encephalon. In an infant, the most obvious sign of hydrocephalus is an abnormal enlargement of the babe's head. In children symptoms tend to be related to high force per unit area and may include nausea, vomiting, headache and vision problems.
In young and middle aged adults symptoms well-nigh often include dizziness and vision bug. In older adults with normal pressure hydrocephalus the symptoms are more likely to be loss of function in three master areas: walking, thinking and bladder control.
Infants
Common signs and symptoms of hydrocephalus in infants include:
Changes in the head
- An unusually big caput
- A rapid increase in the size of the head
- A jutting or tense soft spot (fontanel) on the summit of the head
Physical signs and symptoms
- Vomiting
- Sleepiness
- Irritability
- Poor feeding
- Seizures
- Optics fixed downwards (sunsetting of the eyes)
- Deficits in muscle tone and strength
- Poor responsiveness to touch
- Poor growth
Toddlers and older children
Among toddlers and older children, signs and symptoms may include:
Physical signs and symptoms
- Headache
- Blurred or double vision
- Eyes fixed downwards (sunsetting of optics)
- Abnormal enlargement of a toddler'due south caput
- Sleepiness or languor
- Nausea or vomiting
- Unstable balance
- Poor coordination
- Poor ambition
- Seizures
- Urinary incontinence
Behavioral and cognitive changes
- Irritability
- Alter in personality
- Decline in school performance
- Delays or problems with previously acquired skills, such every bit walking or talking
Young and Centre Aged Adults
- Chronic headaches
- Difficulty walking/gait disturbances
- Cerebral challenges or complaints
- Urinary urgency or incontinence
- Dumb vision
- Turn down in retentiveness, concentration and other thinking skills that may affect chore performance
Older Adults (normal pressure hydrocephalus)
- Difficulty walking/gait disturbances, often described as a shuffling gait or the feeling of the anxiety beingness stuck
- Cognitive challenges/mild dementia/memory loss
- Urinary urgency or incontinence
- Poor coordination or balance
Hydrocephalus diagnosis
The most mutual initial diagnostic test to make up one's mind hydrocephalus at whatsoever historic period is an image of the brain using CT or MRI to place if the ventricles or spaces within the brain are enlarged. More than tests are oftentimes performed in adults in guild to diagnosis the condition. The decision to club a particular test may depend on the specific clinical situation, likewise equally the preference and experience of the medical squad. Non all of the tests described here are required in society to make a diagnosis.
- Clinical exams to evaluate symptoms consist of an interview and/or concrete neurological examination.
- Brain images to detect enlarged ventricles normally include magnetic resonance imaging (MRI) and computerized tomography (CT).
- CSF tests to predict shunt responsiveness and/or determine shunt pressure include lumbar puncture, external lumbar drainage, measurement of CSF outflow resistance, intracranial pressure (ICP) monitoring and isotopic cisternography.
Neurological exam
The type of neurological examination will depend on a person's age. The neurologist may ask questions and conduct relatively simple tests in the office to gauge muscle condition, movement, well-existence and how well the senses are performance.
Brain imaging
Encephalon imaging tests can prove enlarged ventricles caused by excess cerebrospinal fluid. They may also be used to identify underlying causes of hydrocephalus or other conditions contributing to the symptoms. Imaging tests may include:
- Ultrasound. Ultrasound imaging, which uses high-frequency sound waves to produce images, is often used for an initial assessment for infants considering it'south a relatively uncomplicated, low-risk process. The ultrasound device is placed over the soft spot (fontanel) on the top of a baby's caput. Ultrasound may also discover hydrocephalus prior to birth when the procedure is used during routine prenatal examinations.
- Magnetic resonance imaging (MRI) uses radio waves and a magnetic field to produce detailed 3-D or cross-exclusive images of the encephalon. This test is painless, merely it is noisy and requires lying nonetheless. Children may need balmy sedation for some MRI scans. However, some hospitals use a very fast version of MRI that by and large doesn't require sedation.
- Computerized tomography (CT) browse is a specialized X-ray applied science that can produce cross-sectional views of the brain. Scanning is painless and quick. But this test also requires lying still, and so a child unremarkably receives a mild sedative. Drawbacks to CT scanning include less detailed images than an MRI, and exposure to a small amount of radiations. CT scans for hydrocephalus are normally used only for emergency exams.
Normal pressure level hydrocephalus
Normal pressure hydrocephalus can be difficult to diagnose considering the symptoms come on gradually and are similar to those of more common conditions, such every bit Alzheimer'due south disease.
Information technology's important to make a correct diagnosis because, unlike Alzheimer'south disease, the symptoms of normal pressure hydrocephalus tin be relieved with handling.
Your doctors will appraise:
- how you walk (your gait)
- your mental ability
- symptoms that affect your bladder control, such every bit urinary incontinence
- the appearance of your brain (using scans)
Normal pressure hydrocephalus may exist diagnosed if y'all take walking, mental and float problems, and cerebrospinal fluid (CSF) levels are higher than usual. Nonetheless, you may not have all of the above symptoms.
Farther tests may besides exist carried out to determine whether you would benefit from having surgery, such every bit a:
- lumbar puncture
- lumbar drainage examination
- lumbar infusion exam
Lumbar puncture
A lumbar puncture is a process where a sample of CSF is taken from your lower dorsum. The pressure of the CSF sample is then checked.
Removing some CSF during a lumbar puncture may assistance improve your symptoms.
If this is the example, it'due south a good indication that y'all may benefit from treatment with surgery – see treating hydrocephalus to find out more.
Lumbar drain
Yous may accept a lumbar bleed if a lumbar puncture doesn't meliorate your symptoms.
A tube is inserted between your back basic to drain a large amount of CSF. This is carried out over a few days to run into whether your symptoms amend. The procedure is normally carried out nether local anesthetic.
Lumbar infusion test
During a lumbar infusion examination, fluid is slowly injected into your lower back while measuring the pressure level.
Your body should blot the extra fluid and the pressure should stay low. If your body tin't absorb the extra fluid, the pressure volition ascent, which could betoken normal pressure hydrocephalus and that surgery will be benign.
Hydrocephalus treatment
Hydrocephalus is most oft treated by surgically inserting a shunt organisation. This organization diverts the flow of CSF from the brain and spinal string to another area of your body where information technology can exist absorbed as part of the normal circulatory process.
The increased pressure on the brain caused by hydrocephalus can exist relieved by an performance to insert a ventricular peritoneal shunt (common blazon of hydrocephalus shunt). The shunt drains the fluid from the brain to another part of the body. The hydrocephalus shunt is a long, thin piece of tubing with a one way valve that takes the fluid from the ventricles in the encephalon, under the skin to the abdominal cavity. It is completely within the trunk, just the outline of the tubing can be seen every bit it passes downward the side of the cervix, beneath the ear. A long curlicue of tubing is normally placed in the abdomen to allow the shunt to lengthen as the person grows. The shunt does not cure Hydrocephalus, but by draining the excess fluid it can allow the head and brain to grow usually.
A limited number of individuals tin can be treated with an alternative procedure called third ventriculostomy. In this procedure, a neuroendoscope — a pocket-sized camera that uses cobweb optic technology to visualize small and hard to reach surgical areas — allows a physician to view the ventricular surface. Once the telescopic is guided into position, a small tool makes a tiny pigsty in the flooring of the third ventricle, which allows the CSF to bypass the obstacle and flow toward the site of resorption around the surface of the encephalon.
Having a pediatrician is vital for monitoring of developmental milestones and a skillful family doctor is required into developed life.
Hydrocephalus shunt
A shunt is a flexible but sturdy plastic tube. A shunt arrangement consists of the shunt, a catheter, and a valve. One end of the catheter is placed within a ventricle inside the brain or in the CSF outside the spinal cord. The other stop of the catheter is unremarkably placed inside the abdominal cavity, merely may besides be placed at other sites in the body such every bit a bedroom of the eye or areas around the lung where the CSF can drain and be absorbed. A valve located along the catheter maintains one-way flow and regulates the rate of CSF menstruation.
Hydrocephalus shunt lies completely inside your body, only the outline of the tubing tin can exist seen as it passes down the side of the neck, below the ear. A long coil of tubing is normally placed in the belly to allow the shunt to lengthen equally the person grows. The shunt does not cure hydrocephalus, merely past draining the backlog fluid it can permit the head and encephalon to grow normally.
A shunt is a delicate piece of equipment that can malfunction, commonly by becoming blocked or infected.
It's estimated up to 4 out of 10 shunts will malfunction in the first year after surgery.
Sometimes a scan afterward the operation shows the shunt isn't in the best position, and further surgery is needed to reposition it.
If a baby or child has a shunt fitted, the shunt may become too small as the child grows, and information technology volition need to exist replaced. As most people demand a shunt for the rest of their life, more than than one replacement may be needed.
Bleeding tin can occasionally occur when shunt tubes are positioned. This can upshot in nervus problems, such equally weakness down i side. There is also a small-scale chance of fits after any type of encephalon surgery.
In younger children, particularly babies, cerebrospinal fluid (CSF) can run alongside the shunt rather than downwardly it, and the fluid can leak through the pare wound. Additional stitches will be needed to stop the leak.
Effigy 4. Hydrocephalus shunt
 What problems tin can occur with hydrocephalus shunts?
What problems tin can occur with hydrocephalus shunts?
Shunt systems are imperfect devices. Complications may include mechanical failure, infections, tubing can be blocked, or kinked, breaks and becomes disconnected or if the valve stops working properly, and the demand to lengthen or replace the catheter. Infection tin can also crusade shunt dysfunction. Shunt infection tin occur at any stage, only is more than common just after a new shunt has been inserted or after revision of the shunt. By and large, shunt systems crave monitoring and regular medical follow up. When complications occur, subsequent surgery to replace the failed part or the entire shunt system may be needed.
Hydrocephalus is monitored in the outpatient clinic by the pediatrician, rehabilitation specialist and/or the neurosurgeon. A review of the signs and symptoms of shunt dysfunction is carried out at each dispensary visit.
Some complications can lead to other issues such as overdraining or underdraining. Overdraining occurs when the shunt allows CSF to drain from the ventricles more quickly than it is produced. Overdraining can cause the ventricles to collapse, fierce blood vessels and causing headache, hemorrhage (subdural hematoma), or slit-like ventricles (slit ventricle syndrome). Underdraining occurs when CSF is not removed quickly enough and the symptoms of hydrocephalus recur. Overdrainage and underdrainage of CSF are addressed by adjusting the drainage pressure of the shunt valve; if the shunt has an adjustable pressure valve these changes can exist made by placing a special magnet on the scalp over the valve. In improver to the mutual symptoms of hydrocephalus, infections from a shunt may likewise produce symptoms such as a low-grade fever, soreness of the neck or shoulder muscles, and redness or tenderness forth the shunt tract. When there is reason to suspect that a shunt system is not operation properly (for example, if the symptoms of hydrocephalus return), medical attention should be sought immediately.
The alert signs of shunt dysfunction or infection can include some of the following:
In infants:
- Rapid caput growth (in babies).
- Full,bulging or tense soft spot (fontanel) at the top of the head (present until the skull closes at about 18 months of historic period).
- Swelling and/or pain along the shunt, especially at the side of the neck.
- Unusual irritability
- Nausea and vomiting
- Crossed eyes/sun setting eye
- Periods when the baby stops breathing (apnea) or drowsiness
- Difficulty drinking/swallowing/crying.
In older children:
- Headache
- Visual disturbance (blurred vision)
- Drowsiness
- Loss or decrease of consciousness
- Lethargy.
Less common signs can include:
- Difficulty in walking and inverse mobility (due to weakness, residuum issues, deterioration in sensation worsening of orthopedic problems)
- Memory problems or significant modify in intellectual operation
- Decline in milestones
- Seizures (new or worsening or increased frequency of existing seizures)
- Back pain or worsening scoliosis
- Changes in incontinence
- Hearing sensitivities.
Shunt infection
Shunt infection is also a relatively common complication after shunt surgery. The adventure of infection is around 3-15% and is more than likely to occur during the starting time few months later on surgery.
The signs and symptoms of a shunt infection may include:
- Redness and tenderness along the line of the shunt
- A loftier temperature (fever) of 38 °C (100.iv °F) or above
- Headache
- Airsickness
- Neck stiffness
- Intestinal pain if the shunt drains into your tummy
- Leakage from the shunt wound expanse or tenderness along the tract
- Irritability or sleepiness in babies
Contact your care team immediately if you or your kid has these symptoms.
Antibiotics may be needed to treat the infection and, in some cases, surgery may be required to supersede the shunt.
Shunt alert cards
Shine (of U.k.), the hydrocephalus and spina bifida charity, has produced a serial of shunt warning cards for adults and children. You carry the card with you if you've had a shunt fitted.
The carte is useful in a medical emergency if you have symptoms of a blockage or infection.
The healthcare professionals treating you will exist aware that you have a shunt fitted and will bank check whether this is causing your symptoms.
To utilise for a shunt alert card, you can either fill out a form on the Shine website here: https://world wide web.shinecharity.org.uk/hydrocephalus/taking-care-of-yourself/shuntalertcards
Additional treatments
Some people with hydrocephalus, particularly children, may need additional treatment, depending on the severity of long-term complications of hydrocephalus.
A care squad for children may include a:
- Pediatrician or physiatrist (concrete medicine and rehabilitation doctor), who oversees the treatment programme and medical care
- Pediatric neurologist, who specializes in the diagnosis and treatment of neurological disorders in children
- Occupational therapist, who specializes in therapy to develop everyday skills
- Developmental therapist, who specializes in therapy to help your kid develop age-advisable behaviors, social skills and interpersonal skills
- Mental health provider, such as a psychologist or psychiatrist
- Social worker, who assists the family with accessing services and planning for transitions in care
- Special education teacher, who addresses learning disabilities, determines educational needs and identifies appropriate educational resource
Adults with more-astringent complications also may crave the services of occupational therapists, social workers, specialists in dementia intendance or other medical specialists.
Endoscopic Third Ventriculostomy
A second treatment selection for hydrocephalus is a surgical process chosen endoscopic 3rd ventriculostomy. This same endoscopic 3rd ventriculostomy procedure with the addition of choroid plexus cauterization is available for infants. In the endoscopic third ventriculostomy procedure, an endoscope is used to puncture a membrane in the floor of the tertiary ventricle creating a pathway for CSF flow within the cavities in the brain. This approach is an of import alternative to shunting for obstructive hydrocephalus and may exist useful in other cases every bit well.
The third handling option involves the addition of choroid plexus cauterization with endoscopic tertiary ventriculostomy in infants. The neurosurgeon uses a device to fire or cauterize tissue from the choroid plexus. The choroid plexus is a network of vessels in the ventricles of the brain where cerebrospinal fluid is produced.
The success rate for endoscopic tertiary ventriculostomy or endoscopic 3rd ventriculostomy/choroid plexus cauterization depends upon patient factors such as age, cause of hydrocephalus, and whether at that place is scarring in the fluid space below the floor of the third ventricle. For some patients, the chance for success of the endoscopic third ventriculostomy may be upwardly to 90%; however, for others, endoscopic third ventriculostomy – with the addition of choroid plexus cauterization for infants – may not be recommended because the chances for success are sufficiently low. Your neurosurgeon should be able to provide you with a reliable gauge of the likelihood for success in your item state of affairs prior to the functioning. It's critical that parents and patients sympathize that endoscopic 3rd ventriculostomy is non always a permanent cure for hydrocephalus. Candid communication with your dr. regarding the definition of success is important when considering endoscopic third ventriculostomy.
Complications of endoscopic third ventriculostomy
The endoscopic tertiary ventriculostomy/choroid plexus cauterization process is only bachelor to infants.
The success rate for endoscopic 3rd ventriculostomy or endoscopic 3rd ventriculostomy/choroid plexus cauterization depends upon patient factors such equally age, cause of hydrocephalus, and whether there is scarring in the fluid space below the floor of the third ventricle. For some patients, the chance for success of the endoscopic third ventriculostomy may be up to 90%; however, for others, endoscopic third ventriculostomy – with the improver of choroid plexus cauterization for infants – may not be recommended considering the chances for success are sufficiently low. Your neurosurgeon should be able to provide you lot with a reliable estimate of the likelihood for success in your particular state of affairs prior to the functioning.
The near common complication with these ii procedures is closure of the pathway that is surgically created with endoscopic third ventriculostomy and infection.
- Sudden Pathway Closure with endoscopic third ventriculostomy and endoscopic third ventriculostomy/choroid plexus cauterization
Sudden closure of the pathway created using endoscopic third ventriculostomy can be sudden and life-threatening. Pathway closure occurs in 20 to 50% of patients within v years of the procedure with the great majority of treatment failures occurring within the beginning 6 months of the operation. Although belatedly failures can occur, they are rare, and the ongoing take chances of handling failure over subsequent years is much less than that for patients with shunt-dependence.
Information technology'south critical that parents and patients empathise that endoscopic tertiary ventriculostomy is not a permanent cure for hydrocephalus. Candid communication with your physician regarding the definition of success is important when considering endoscopic third ventriculostomy.
- Infection with endoscopic third ventriculostomy and endoscopic third ventriculostomy/choroid plexus cauterization
Infection occurs in up to less than one percentage of those treated surgically with endoscopic third ventriculostomy or endoscopic tertiary ventriculostomy/choroid plexus cauterization procedures.
- Fever and Bleeding with endoscopic third ventriculostomy and endoscopic tertiary ventriculostomy/choroid plexus cauterization
With new technologies the risks of endoscopic third ventriculostomy have been minimized, however there are all the same potential complications including fever and bleeding. Attempts to perforate or create an opening in the ventricular floor can lead to haemorrhage, as can damage to ventricular walls or perforation of the basilar artery. Big bleeds due to vessel injury nether the 3rd ventricle tin be catastrophic, but they are rare.
Other complications from endoscopic 3rd ventriculostomy include brusk-term memory loss, since the process may affect the hypothalamus and the areas of the mammillary body which are responsible for memory. This is typically a temporary complication. Endocrinologic irregularities can occur following endoscopic third ventriculostomy and endoscopic third ventriculostomy/choroid plexus cauterization equally a result of the minor opening in the area of the third ventricle which is responsible for some hormonal function. This complication is also often short lived.
Hydrocephalus Shunt and Endoscopic Third Ventriculostomy Complications
When things are going well, information technology's easy to put the concerns about hydrocephalus and the complications that come up with information technology out of your mind. However, information technology's critical to understand the signs and symptoms of a shunt failure or the closure of an endoscopic third ventriculostomy. Seeing your doctor or visiting the Emergency Department, fifty-fifty if symptoms are not ultimately related to hydrocephalus, the shunt, endoscopic third ventriculostomy or endoscopic tertiary ventriculostomy/choroid plexus cauterization, is the correct choice. Seeking immediate medical attending can place a resolvable complication and enable you or your family fellow member to avert encephalon impairment or fifty-fifty death, especially in children.
Symptoms of shunt malfunction or endoscopic tertiary ventriculostomy closure vary considerably from person to person, merely recurring failures tend to have similar symptoms for a detail person. When an precipitous malfunction occurs, symptoms can develop very speedily potentially leading to coma and mayhap expiry. In infants and toddlers, it's important to be aware that medication with a side effect of drowsiness tin mimic or mask signs of shunt malfunction or endoscopic third ventriculostomy closure and should be used with caution in those with hydrocephalus, peculiarly infants and young children.
Infants
- Enlargement of baby's head
- Fontanel full and tense when infant is upright and quiet
- Prominent scalp veins
- Swelling along shunt tract
- Airsickness
- Sleepiness
- Irritability
- Down deviation of optics
- Less interest in feeding
- Fever, potentially present with shunt failure or infection
- Redness along shunt tract, potentially present with shunt failure or infection
Toddlers
- Enlargement of head
- Swelling along shunt tract
- Vomiting
- Headache
- Sleepiness
- Irritability
- Loss of previous abilities (sensory or motor function)
- Fever, potentially present with shunt failure or infection
- Redness forth shunt tract, potentially present with shunt failure or infection
Children and Adults
- Vomiting
- Headache
- Vision problems
- Irritability and/or tiredness
- Swelling forth shunt tract
- Personality modify
- Loss of coordination of rest
- Difficulty waking upwards or staying awake (this symptom requires urgent attention as information technology can potentially lead to a coma)
- Decline in academic or task functioning
- Fever, potentially present with shunt failure or infection
- Redness along shunt tract, potentially present with shunt failure or infection
Older Adults with Normal Force per unit area Hydrocephalus
People who are diagnosed and treated in adulthood, including those with Normal Pressure Hydrocephalus, tend to revert to the symptoms they experienced earlier initial treatment when they are experiencing a shunt malfunction.
- Difficulty walking/Gait disturbances
- Cognitive challenges/Balmy dementia
- Urinary Urgency or incontinence
- Fever (sign of shunt failure or infection)
- Redness forth the shunt tract (sign of shunt failure or infection)
Normal force per unit area hydrocephalus
Normal pressure hydrocephalus, which usually affects older people, can sometimes be treated with a shunt, although not everyone with the status volition do good from shunt surgery.
As there's a risk of complications with shunt surgery, you'll need tests to assess whether the potential benefits of surgery outweigh the risks.
Lumbar drainage or a lumbar infusion test, or both, can be used to determine whether shunt surgery volition benefit you lot.
Coping and back up
With the help of rehabilitative therapies and educational interventions, many people with hydrocephalus live with few limitations.
In that location are many resources available to provide emotional and medical support as y'all parent a child with hydrocephalus. Children with developmental issues due to hydrocephalus may be eligible for authorities-sponsored health care and other support services. Check with your land or county social services agency.
Hospitals and voluntary organizations serving people with disabilities are good resource for emotional and practical back up, every bit are doctors and nurses. Ask these resources to help y'all connect with other families who are coping with hydrocephalus.
Adults living with hydrocephalus may find valuable information and support from organizations dedicated to hydrocephalus instruction and support, such as the Hydrocephalus Association https://www.hydroassoc.org/.
Source: https://healthjade.com/hydrocephalus/
{kind=link}
Post a Comment for "Can a Baby With Hydrocephalus Lead a Normal Life?"